
Online referral form
Please use the form below to send us a referral. Alternatively, you may send your referral to reception@goortho.com.au.
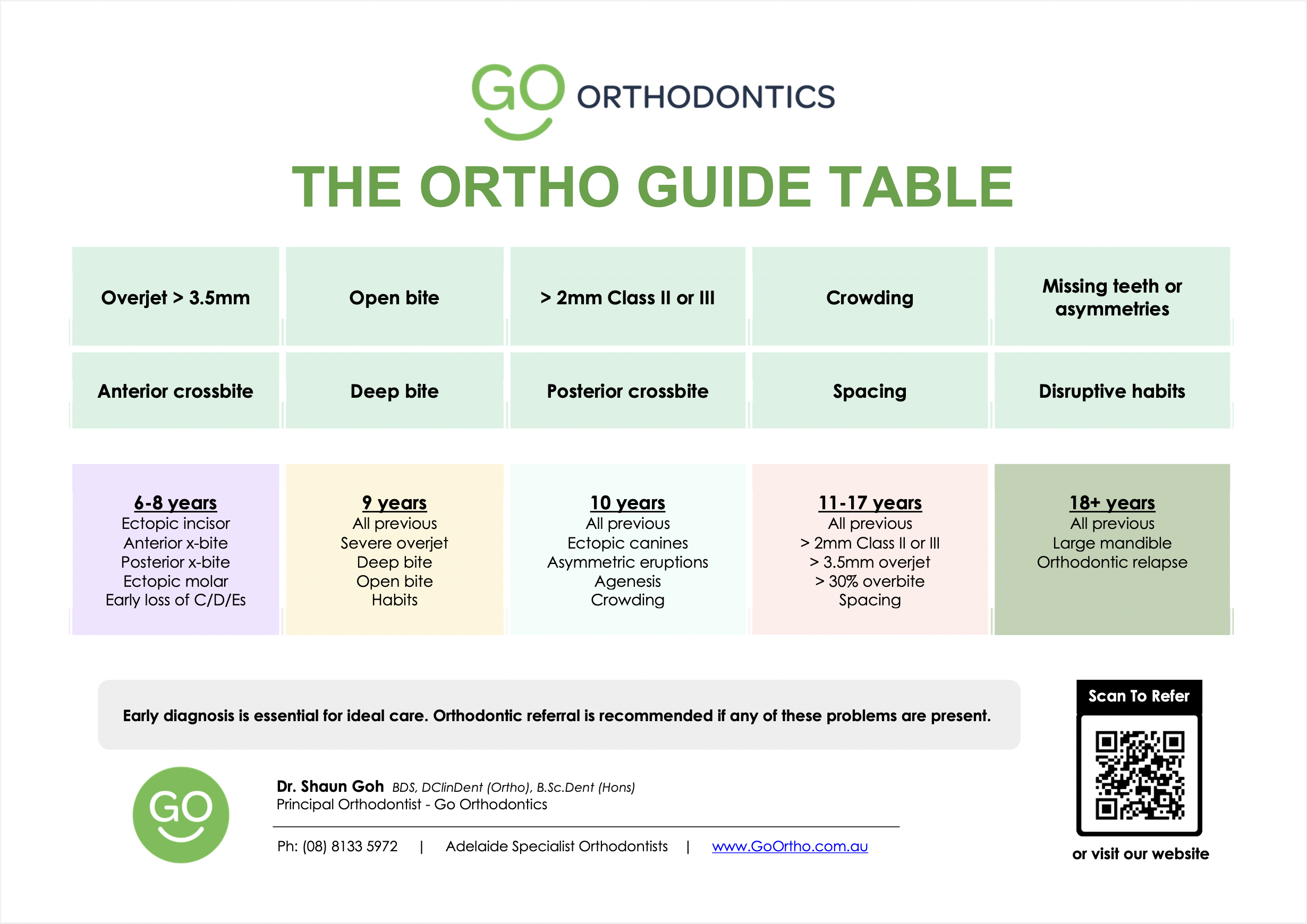
Go Orthodontics Problems Guide
")
Please use the form below to send us a referral. Alternatively, you may send your referral to reception@goortho.com.au.

Dental Assistant

Treatment Coordinator
")
Dental Assistant
Ashlee is our dental assistant! She loves seeing patients overjoyed about their orthodontic results. Ashlee brings an incredible amount of fun to Go Orthodontics!

Practice Manager

Oral Health Therapist
Vanessa Tu is our oral health therapist who works alongside Dr Goh in providing the highest standard of orthodontic care. Vanessa is an expert on oral hygiene with braces and will be able to show you the best way to care for your appliances. She is gentle and loves to get to know all our patients.

Specialist Orthodontist and Director
Dr. Shaun Goh is a specialist orthodontist and the director of Go Orthodontics. He has over a decade of experience as a specialist orthodontist and dental surgeon.
Dr. Goh obtained his undergraduate dental degree (BDS) with concurrent honours at Adelaide University in 2012, his National Dental Board Exams (Canada) in 2014, his Master Implant Program at the Brener Implant Institute (Sydney) in 2016 and his postgraduate Doctor of Clinical Dentistry (DClinDent Orthodontics) at Adelaide University in 2021.
Dr. Goh is a consultant at Adelaide University Dental Hospital where he teaches future orthodontists during their post-graduate specialist training. He is also a committee chairperson in the Australia Society of Orthodontists.
Dr. Goh has taught numerous dentists on the importance of early diagnosis and its influence on improved orthodontic treatment. He loves orthodontics as he gets to resolve biological puzzles everyday and transform patients’ lives with amazing life-long smiles. He practices with a “Shokunin” philosophy – where he employs the latest techniques and a relentless pursuit of perfection in the craft of orthodontics.
Dr. Goh has published multiple scientific papers on Invisalign in the highest ranked orthodontic journal – American Journal of Orthodontics and Dentofacial Orthopaedics. He has worn multiple awards including Excellence in the Royal College of Dental Surgeons’ Primary Examinations in 2015, the best research presentation in Doctor of Clinical Dentistry at Adelaide University in 2021 and best postgraduate case presentation at the Australian and New Zealand Society of Paediatric Dentistry in 2021.
Outside of orthodontics, he has a growing family with two young sons and two cocker spaniels. He loves mountain biking and surfing.
{kind=link}